Thakurdas Bang was a freedom fighter, an economist, and one of those men whose biography seems impossibly interwoven with the story of a young nation. In Nagpur, he taught economics at a college founded by Gandhi’s associates. During the Quit India Movement of 1942, he was imprisoned for two years. When he emerged, the air was thick with the imminence of independence. The Indian government offered him a scholarship to pursue graduate studies in economics in the United States.
Thakurdas Bang
Before leaving, Thakurdas Bang traveled to Sevagram to seek Gandhi’s blessings. He placed his admission papers before Bapu and said, “I wish to go to America for a doctorate in economics. I want your blessings.” Gandhi looked at him and said, gently but unmistakably, “If you want to study economics, go to the villages. Live with the poor. Learn from them.” There was no room for argument. Bang tore up his admission papers and instead went to live in a village near Sevagram. He would go on to work closely with Vinoba Bhave in the Bhoodan and Gramdan movements and later with Jayaprakash Narayan’s Sarvodaya Movement.
He and his wife raised two sons: Ashok and Abhay. The elder, Ashok, chose agriculture as his life’s work; the younger, Abhay, chose health. Abhay was born in Sevagram in 1950, and until the ninth grade, was educated in the Gandhian system of Nai Talim, where the school curriculum was inseparable from life itself.
As part of this education, Abhay was allotted a small plot of land. He was expected to cultivate it, harvest the produce, and sell it in the market—an early lesson in livelihood. He chose to grow eggplant. Because chemical fertilizers were not permitted, he gathered cow dung and urine from the goshala and used the same as fertiliser. Too much enthusiasm, however, produced eggplants of such prodigious size that no buyer trusted them. He carried the unsold vegetables home, chastened. Later he would say it was his first lesson in economics: production must consider the needs and perceptions of the consumer.
One day, while walking home from school along a hill path, the brothers spoke about the future. Their conversation ended in a pact: Ashok would study agriculture to serve poor farmers, and Abhay would become a doctor to serve the sick.
Both Ashok and Abhay kept their promise. Abhay graduated at the top of his class from Nagpur Medical College, then again from his postgraduate program in general medicine. As their classmates left for advanced degrees and prosperous futures abroad, Abhay wrestled with the question he had carried since childhood—whether to follow the tide or remain true to service. After long reflection, he chose service.
He married Rani, a fellow physician who specialised in obstetrics and gynecology. Together they joined Ashok in running Chetna, an organization providing free services and medical care for the rural poor. But their ambitions were larger. They left for Johns Hopkins University to pursue master’s degree in public health.

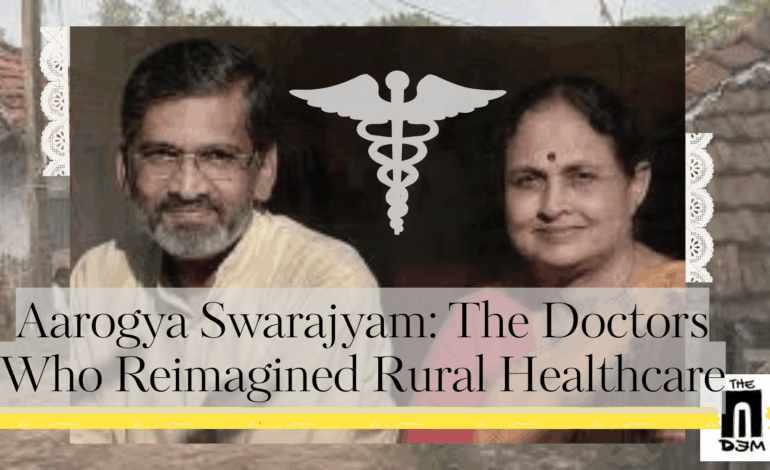
Abhay and Rani Bang
When they returned to India, they headed not to any booming metropolis but to one of the country’s most remote districts: Gadchiroli, in eastern Maharashtra, part of the dense forest belt of Dandakaranya. Seventy percent forested, more than half populated by the Gond tribe, and nearly a thousand kilometers from Mumbai, Gadchiroli was among India’s most underdeveloped regions.
There, the Bangs founded SEARCH—Society for Education, Action and Research in Community Health. The website of Search has this talisman from Gandhi:
“I shall give you a talisman. When faced with a dilemma as to your next step, remember the most wretched and vulnerable human being you ever saw. The step you contemplate should help him.” This became their compass.
SEARCH Logo
When they arrived, the tribal population remained wary of modern medicine. To bridge that distance, Abhay and Rani organised a jatra—a community festival where they listened, not lectured. At the end of it, they proposed a hospital for the Gond community, built with the participation of the people themselves. The Gonds responded with enthusiasm and specificity. The hospital must resemble a home, not a towering institution. It must not be multi-storied. At the entrance, there must be a temple for Ma Danteshwari, the reigning deity of the forests. And the hospital must be named the Ma Danteshwari dawa Khana.

Maa Danteshwari Clinic (Depiction)
In that same gathering, four problems emerged as the community’s most urgent: malaria, alcoholism, infant mortality, and maternal health issues.
The Bangs decided to begin with infant mortality. In 1988, the infant death rate in the region was 121 per 1,000 births, one of the highest. They began with the simplest act: keeping their ear to the ground. They collected data from Gond villages, speaking to mothers who had lost infants. They compiled the first verbal autopsies—imperfect but invaluable—because in a place without records, even an imperfect window into truth is a beginning.
Their findings were stark. In the first month of life alone, 39% of deaths occurred. Pneumonia, diarrhoea, malaria, and vaccine-preventable diseases were major culprits. Maternal malnutrition compounded the crisis. Perhaps most significantly, most births occurred at home, in dark mud huts where mother and child were confined for 30 days due to traditional beliefs about evil eyes. Ventilation was poor and hygiene, worse.
More than half of first-month deaths were due to infections. Another 20% were caused by birth asphyxia. Fifteen percent were premature infants with low birth weight. The Bangs realised that the first month—the neonatal period—was the battleground.
They selected 39 women from 39 villages—not for their education, but for their compassion, steadiness, and willingness to learn. They were named Arogya Doots—health messengers.
If a baby survived the first month, survival odds improved dramatically. So the Bangs trained the Arogya Doots rigorously in hygiene, infection detection, breastfeeding, and basic life-saving measures. Thus, was born the concept of Home-Based Neonatal Care (HBNC).
The methods were simple and rooted in village life. Health workers visited pregnant women with illustrated manuals explaining nutrition, hygiene, and care. They assisted with childbirth and monitored newborns, recording temperature, weight, and symptoms.
To detect infection—a delicate art even for specialists—the Bangs trained the women so effectively that, as Abhay later wrote, they became as competent as neonatologists at Harvard, sometimes more so. This was not hyperbole—their findings were published in The Lancet.
A critical problem in neo-natal care was administering antibiotics safely. Gentamicin, a life-saving injectable drug, had to be dosed precisely according to a newborn’s weight. The solution arrived almost serendipitously: insulin syringes, pre-sterilized and calibrated for small doses which are normally used for diabetics. Their fine needles were perfect for the newborns. With careful training, the Arogya Doots could administer weight-appropriate doses.
But this raised ethical and legal questions. Indian medical law does not permit non-professionals to administer injections. To address this, the Bangs invited the country’s foremost paediatricians—including Dr. Meharban Singh of AIIMS and Ramesh Poddar, president of the Asian Congress of Paediatrics—to evaluate their program and test the Arogya Doots.
After three days of rigorous assessment, Dr. Meharban Singh declared, “These women of Gadchiroli, who walk like ordinary villagers, know more about newborn care than the paediatricians we train at AIIMS.” The expert panel approved the program happily.
The intervention was launched in 39 villages, with 47 neighboring villages (served by government facilities) as controls. After eight years, the results were striking. Deaths due to low birth weight dropped from 11.3% to 4.9%. Prematurity-related deaths fell from 33.3% to 10.1%. Infection deaths from 18.5% to 6.9%. Birth asphyxia deaths from 38.5% to 20.2%. Neonatal mortality itself plummeted from 60% to 22%. By contrast, the control villages saw no improvement; their infant mortality rose slightly.
The district’s overall infant mortality dropped from 120 to 30—below India’s national average and approaching Kerala’s celebrated levels.
This revolution happened not with fleets of doctors or costly equipment, but by two physicians, 39 village women, basic kits costing 1,500 rupees each, and 28 days of training. The cost of saving a life averaged 350 rupees. Few healthcare interventions anywhere in the world could claim such efficiency.
“Science,” Abhay Bang says, “is the best vaccine against human suffering.” His dream was not to build dependency on doctors, but to empower communities to achieve Aarogya Swaraj—health self-rule.
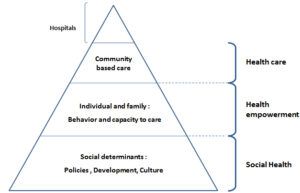
Pyramid to understand SEARCH’s Mission
Inspired by the success in Gadchiroli, the Government of India launched the nationwide ASHA (Accredited Social Health Activist) program in 2005. The whole country benefitted by the success HBNC of Gadchiroli.
The story did not end with neonatal care. The Gond women urged Rani Bang to help them confront alcoholism—a scourge ravaging their families. Under the leadership of Bangs and support, the community waged a determined campaign that culminated in the closure of all the 60 licensed liquor shops in the district.
The world took notice. HBNC was recognised by the World Health Organization as one of the most effective public-health interventions for developing countries. It spread to Nepal, Bangladesh, and later to several African nations, in fact becoming the national health strategy of Ethiopia.
To celebrate its 180 years of publication, The Lancet has showcased discoveries that changed the world—Ronald Ross’s work on malaria transmission, the identification of cholera bacteria, the invention of insulin and penicillin etc. And Bangs’ landmark initiative of Home Based Neonatal Care (HBNC) and its success was placed alongside with the above inventions as an important healthcare initiative which benefitted humanity.
Rani then turned to another silent epidemic: gynaecological disorders among Gond women. In her surveys, 92% of women reported symptoms—pain, infections, sexually transmitted diseases—that had gone unacknowledged for generations. Through community meetings, training of the rural health workers, and culturally sensitive engagement, she helped transform women’s health from a private burden into a public conversation.

Abhay and Rani Bang in a session for women and children
It was a reminder—quiet, yet powerful—that sometimes the most transformative healthcare breakthroughs do not emerge from laboratories or gleaming hospitals, but from mud huts in forgotten forests, carried forward by women with picture books and insulin syringes. A reminder that Gandhian ideals, when translated into rigorous science, can certainly reshape the world.
This is Aarogya Swaraj. This is health in the people’s hands.
Aarogya Swaraj and SEARCH’s Motives
Known as the Father of the White Revolution, the mind behind India becoming the world’s largest milk producer- Verghese Kurien’s co-operative economy model has stood the test of time amidst dominantly capitalist modes of production. With welfare and equity as the drivers instead of mere profit, Co-operatives showcase how alternate models can balance dignity of labor with profitability.
Balasubramaniam Muthusamy writes about the history of AMUL, the story that led Kurien to innovate a mechanism whereby cottage industries are core participants in modern market systems. It is a success story for Gandhian economics. Production by the masses, not mass production. This article is the second installment of the series on Gandhian Economics.
The Series on Gandhian Economics –
Gandhian Economics- Ideas, Misconceptions, and Evidence
Verghese Kurien- An Unsung Epic